The World Professional Association for Transgender Health (WPATH) just held their 25th symposium, a biennial event where professionals involved in transgender health and trans activists can come together to learn and network.
I had attended the last meeting in 2016 in Amsterdam, and found it a fascinating experience – a concentrated mix of science, activism, opinion, politics and diversity, and a great way to see what was going around the world in trans health – so I decided I would go again.
WPATH has been around for a long time, originally known as the Harry Benjamin Gender Identity Disorder Association, founded in 1978, and changing its name in 2007. WPATH is best known for its Standards of Care (SOC), a large document freely available online, which is designed to provide guidelines for the psychological and medical management of transgender people. The SOC is now in its 7th incarnation, and an 8th version is currently underway. The SOC have been heavily criticized in the past for being too conservative, promoting a gate-keeping approach to trans access to hormones and surgery, and being rather “US-centric”. SOC7 went some way towards addressing these criticisms, including relaxing the recommendations regarding psychiatric assessment prior to medical therapy. There is great hope that SOC8 will involve a larger revision of the entire guidelines, with more emphasis on trans people being able to access both medical and surgical therapy as a basic human right. I will come back to SOC8 later.
The conference was held at the Hilton Hotel in Buenos Aires, and my trek every day from my (several fewer stars) not-the-Hilton hotel took me through quite a dodgy part of the city – the contrast with the Hilton environment was stark and reminded me that this was a poor country. I also wondered how local people could afford the exorbitant conference registration, and later discovered that they couldn’t.
So what happened at WPATH2018? There were several streams of presentations, divided into medical, mental health, ethics, child and youth, surgical, sexual health and fertility. One of the great difficulties I found at this conference was being able to get to all the sessions I had earmarked. For such an expensive conference, it was not well organized. There were many concurrent sessions, and attendees were not provided with abstracts, which made it difficult to know how relevant a session would be, and I had to make my decisions based on the titles and who was presenting. As a result I missed some quite important talks, and did on occasion end up in a room listening to something that was not of interest to me (I mean, I’m sure that intra-nipple distance after top surgery is a fascinating topic for surgeons, but doesn’t really inform my practice!).
I’m going to concentrate first of all on the medical sessions that were relevant to me as a primary care provider in the community, and I will finish up with a summary of some of the more controversial discussions that took place at the end of the conference(one of the controversies is that there was not enough time for proper discussion!).
MEDICAL RISKS OF HRT
There were a variety of presentations on medical outcomes related to HRT.
Mortality
Previous poorly controlled studies have shown an increased risk of suicide and cardiovascular-related mortality in transgender people on HRT. Christel de Blok from VUMC in Amsterdam presented a retrospective analysis spanning 20 years of people attending the clinic up until 2016, and compared them with age-matched controls.
There was an increased mortality in trans women, which was explained by suicide and AIDS. There was an increased mortality in trans men due to unknown causes. I found this data rather unhelpful – it would be good to have a greater inspection of the causes of mortality and whether any of them were actually related to HRT. It seems in the trans women cohort at least that the deaths were not linked to HRT, but rather to mental health problems and complications of HIV infection. I would imagine that with advances in the management of HIV the mortality from this would drop significantly if we looked at a prospective cohort from say 2010 (she is planning to do this by the way). Also the increasing acceptance by society and improved access to care might see a reduced rate of suicide in this group.
Other presentations attempted to drill down further into specific adverse effects of HRT.
Cardiovascular Events
There was agreement from different presenters that the only clear cardiovascular signal was a 2 to 4 fold increase in venous thromboembolism (blood clots), and I was disappointed to see very little data related to different forms of oestrogen, other than statements that risk was mostly related to oral ethinyl oestradiol or oral oestradiol valerate, especially if progesterone was also taken, and that there was no risk with trans-dermal oestrogen.
One issue that came up was what cardiovascular risk calculator to use for our trans patients, ie should we be using the female calculator for trans women? Currently we don’t have evidence to inform this decision.
Another question without an answer is whether primary prevention of cardiovascular outcomes with aspirin or statins should be considered in trans women on HRT.
Bone Density and Fracture Risk
There are questions about how HRT may affect bone density in both trans men and trans women. Certainly we know that in cis women HRT initiated at menopause has a protective effect on bone density and fracture risk.
There are many variables that may affect bone density, including hormone levels, any periods of time off hormones, activity levels, whether there has been gonadectomy (removal of ovaries or testes), family history, smoking and age.
Chantal Wiepjes presented fracture data on a large cohort of almost 7000 people over a 40 year period. Refreshingly she was able to show that the only increased risk of fracture appeared to be in older trans women who were smokers, and that in the group as a whole there was no increased risk of fracture.
Another study examined change in bone mineral density (BMD) over the 1st 10 years of HRT. The findings were that most people’s BMD was the same as baseline after 10 years. BMD was slightly lower in trans women who had been on lower doses of oestrogen, but was slightly higher in older trans men. They also found that 14% of trans women had osteoporosis before even commencing HRT.
These findings suggest that regular BMD measurements in the 1st 10 years of HRT are unnecessary, but that baseline measurement should be considered especially in older trans women who are smokers.
Breast Cancer Risk
The lifetime background incidence of breast cancer is 1/8 for cis women, and 1/1000 for cis men, and most is oestrogen receptor positive.
Christel de Blok looked at published cases of breast cancer in trans individuals, and found the rate to be similar to the cis male rate.
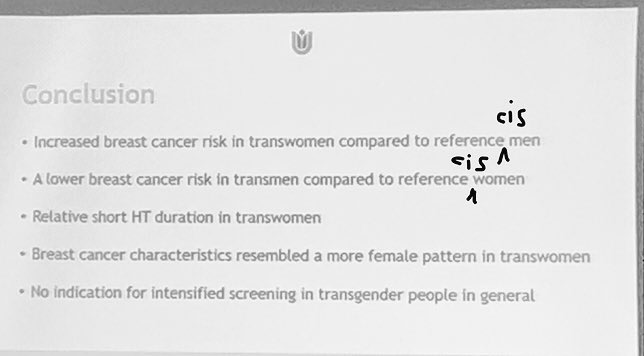
She then went on to examine her large cohort in the Netherlands, and found the breast cancer rate to be reported at 43 cases per 100,000 person years. Overall there was a younger age at the time of diagnosis. There was an increased risk in trans women compared with cis men, and a decreased risk in trans men compared with cis women.
I would have liked to see the data presented differently, with trans women compared with cis women, and trans men compared with cis men, as I think this would have been more useful when talking to patients and deciding on screening algorithms.
There was a fabulously edifying moment when Ukraine trans activist Fritz stood up and demanded that presenters stopped saying “trans women” vs “women” – it should be trans and cis, because trans women are women too! I and many people in the room had definitely been feeling uncomfortable with some of the language being used to present data, and Fritz summed it up nicely. Here is my edited version of the summary slide:
Lipids and Visceral Fat Changes
Everyone is always interested on the likelihood of weight gain with hormones, so it was interesting to look at results from a multicentre prospective study presented by Maartje Klaver from the Netherlands. You can see in the results table below that there was a 21% increase in total body fat in trans women, and this was more marked in women with a lower BMI to begin with. Happily the change was not in visceral fat which is the type of fat linked to greater medical risk. The trans men had a drop in total body fat and an increase in lean body mass, which I think illustrates how we shouldn’t rely on weight alone as a measure of health.
Cholesterol changes after a year on HRT were not earth-shattering – a slight drop in lipids for trans women, and a slight increase in LDL and triglycerides for trans men. The women’s insulin resistance went up, a little and the men’s went down a little.
Haematocrit and Testosterone
We know that testosterone increases the haematocrit, and in trans men it will adjust into the male reference range within 3 months of starting treatment. A presentation by Justine Defreyne from Ghent University showed that testosterone undecanoate had a lesser effect than injectable short-acting testosterone esters, and testosterone gel was somewhere in the middle.
The mechanism appears to be an increase in erythropoietin production and increased iron availability and iron turnover. The concern is that this leads to an increase in risk of blood clots. The generally accepted cut-off for the haematocrit being too high is 0.54, and the recommendation is to switch testosterones or adjust the dose downwards.
HORMONE TREATMENT FOR NON-BINARY PEOPLE
I missed most of this session due to the poor timetabling of the conference. I wish I had known it was on instead of stumbling across it halfway through.
Here’s a summary of what I caught:
There is no current literature on hormonal treatment for non0binary people, and more research is needed. There is no data on long-term outcomes.
For non-binary people AMAB:
Using GnRH analogues to suppress testosterone
- up to 18 mth has no impact on BMD
- after 18 mth BMD will begin to decline
- will result in far less breast growth than either cyproterone or spironolactone
Clinical approach to partial feminization
- low dose oestrogen alone will not suppress testicular function
- breast development is possible at all oestrogen doses
- muscle mass drops once T<10 nmol/l
- sexual dysfunction once T<5 nmol/l
- body hair reduction at T<3 nmol/l
For non-binary people AFAB:
Clinical approach to partial masculinization
- can rely on reliable pattern of changes – voice, facial hair – and stop androgen therapy at the desired stage of change, or switch to low dose
- body hair patterns will regress to female, but not facial hair
- clitoral growth will not regress
- menstruation will return
- beware BMD drop if using low dose T, could potentially use raloxifene for bone protection
PERIOPERATIVE ISSUES FOR TRANS MEN
This session covered some common issues for trans men:
- Atrophic vaginal tissue is more susceptible to trauma, bacterial vaginosis, and perhaps cystitis
- Vaginal cuff (the top part of the vagina that is stitched closed during hysterectomy) may take longer to heal in the low oestrogen state
- Use of oestrogen cream post-operatively for hysterectomy can decrease bleeding and increase healing times
- Pelvic pain due to pelvic floor muscle spasm can be made worse by hysterectomy
- Post-orgasm pain is common, multifactorial, and very little published literature exists
- Pelvic pain can be related to dips in testosterone level
- If conserving ovaries for later egg harvest, consider salpingectomy (as most ovarian cancers start in the tubes)
- In the US there is concern about trans men losing access to testosterone in the future (worst case scenario in the Handmaid’s Tale diorama we are currently witnessing) so conserving ovaries may be important for maintenance of bone health if no T on board
THE NEOVAGINA
This is one of my favourite topics, not least because there’s so much we don’t know about it! Honestly they could have had an entire symposium and panel discussion on this, rather than the poultry 10 minutes it was allotted, with no time for discussion.
Firstly, the microbiome of the neovagina, ie the bacterial environment, is very different to the cis vagina. There are no lactobacilli, which are the cornerstone of vaginal health in the cis female. But don’t bother trying to put some in there, they won’t survive, as the tissue is the wrong type and the pH is too high.
If discharge develops, it’s important to consider what activity is taking place – if someone is having both vaginal and anal sex, then coliform bacteria growing on a swab may simply represent colonization rather than infection, and may not need to be treated.
If a swab shows Gardnerella or BV type organisms, it may not be necessary to treat for this either if there are no symptoms of note.
Bleeding or pain should necessitate an examination (incidentally an anoscope is a much better instrument that a vaginal speculum for examining the neovagina) – if they are not long post surgery there may be some granulation tissue that needs attending to, but it’s also important to consider STIs and if any lesion is present don’t forget that HSV (herpes) can infect the epithelium of the neovagina.
MISCELLANY
When to stop oestrogen pre-surgery?
- currently surgeons routinely ask women to stop oestrogen 4 to 6 weeks prior to their gender affirmation surgery
- there is absolutely no evidence base for this
- stopping E for such a long time is problematic and may lead to harm
- some women resume it because they feel so bad off it after a while
- some women take up smoking again to help them cope, which is probably worse for postoperative outcomes
Chest Dysphoria Scale
This absolutely brilliant scoring tool for dysphoria in trans men was described by Johanna Olson-Kennedy, and has been published in JAMA Paeds
It measures dysphoria in 4 domains:
Recreational: I avoid swimming in public or going to the beach because of my chest
Social: Dating and intimacy is difficult due to my chest
Physical: I avoid going to the doctor due to my chest
Emotional: I feel like my life hasn’t started yet because of my chest
CONTROVERSY
And finally, as promised, the bit where attendees got their hands on the microphone! At the final session of the conference, the SOC8 chapter leads all had a turn telling us what their content is likely to cover. It was exciting to hear about what might change in SOC8, but to be honest there was not a lot of discussion of content, which was pretty disappointing. As there are 15 chapters this all took quite a long time, and involved a lot of clapping and back-patting, but once it was over, the session was opened up to the audience (it was a packed auditorium), and judging by the number of hands that shot up in the air, I would estimate that WPATH could have given at least 3 hours just to this alone. Thirty minutes was simply not enough time to allow everyone a voice, and I hope that WPATH takes this on board and allows the attendees more time for discussion next time. In fact, I would say that the whole conference needed more time for panel discussions and audience participation.
Some themes which arose:
- WPATH is too US-centric, with very little input from other countries
- one South African doctor stood up to complain that his country feels largely ignored by WPATH, and despite managing a huge cohort of patients for many years he ahs not been able to become a SOC contributor despite repeatedly applying
- Prominent US trans surgeon Marci Bowers spent a good deal of time berating WPATH for having such proscriptive guidelines when it comes to adolescents and surgery, and advocated for the right of adolescents who have been on cross-sex hormones for years to be allowed to have surgery before turning 18 (there was quite some applause in the room after she sat down)
- a local Argentinian activist stood up and accused WPATH of being racist in that they had not widely advertised the session devoted to the new Argentinian governmental recognition of non-binary gender, and the only attendees were other local people – in fact, such an important and momentous change should have been given a plenary in my opinion, which would have allowed the entire conference to hear about how it was achieved.






2 Comments »