HIV
CROI 2026 HIV/STI Treatment and Prevention Update
Last month I attended CROI, the large scientific virology meeting which focuses on HIV, held every year in the US, and I wanted to give you an update on the […]
 Dr Fiona Bisshop
Dr Fiona Bisshop
HIV Doctor,Trans Health Advocate, LGBTI Health Provider, Writer for QNews as "Doc Q"

Last month I attended CROI, the large scientific virology meeting which focuses on HIV, held every year in the US, and I wanted to give you an update on the […]
Last month I attended CROI, the large scientific virology meeting which focuses on HIV, held every year in the US, and I wanted to give you an update on the latest research into HIV and STI treatment and prevention.

This year the conference was in Denver, Colorado. Yes, I braved the US, even though I was fearful that the border officer would inspect my phone and social media presence, then promptly turn me around. But it didn’t happen, I waltzed on through and headed for the snowy north. They call Denver the Mile High city due to its elevation above sea level, and the nearness to snow-covered mountains is honestly the main highlight of Denver. I couldn’t help taking a little side trip to Boulder to do a short hike at the base of the Flatirons, accompanied by my very good friends Prof Chloe Orkin from St Mary’s Hospital London, and Dr Mark O’Reilly from East Sydney Doctors. That mile above really hits you by the way! I was quite surprised at my apparent lack of fitness walking up the mountain trail, until I realised I was probably a little low on the old oxygen! Luckily no bears were encountered on the way.


OK, down to the serious business of the conference. The backpack! This year’s backpack had mixed reviews, but I liked it. The Rocky Mountains patch was a nice addition!

OK, truly serious now. The impact of current US government cuts to funding for treatment and research have been huge and far reaching. When they are finally reversed it will take many years to claw back the gains in HIV prevention and mortality around the globe. And again this year many scientists and clinicians could not attend to present their work due to the travel bans imposed by the US on their countries.
It’s estimated that since the funding cuts to USAID and PEPFAR, there had been an extra 130,000 deaths in 2025, including 13.000 children, and by 2029 there will have been 6-10 million new infections and an extra 14 million deaths worldwide if funding is not restored.
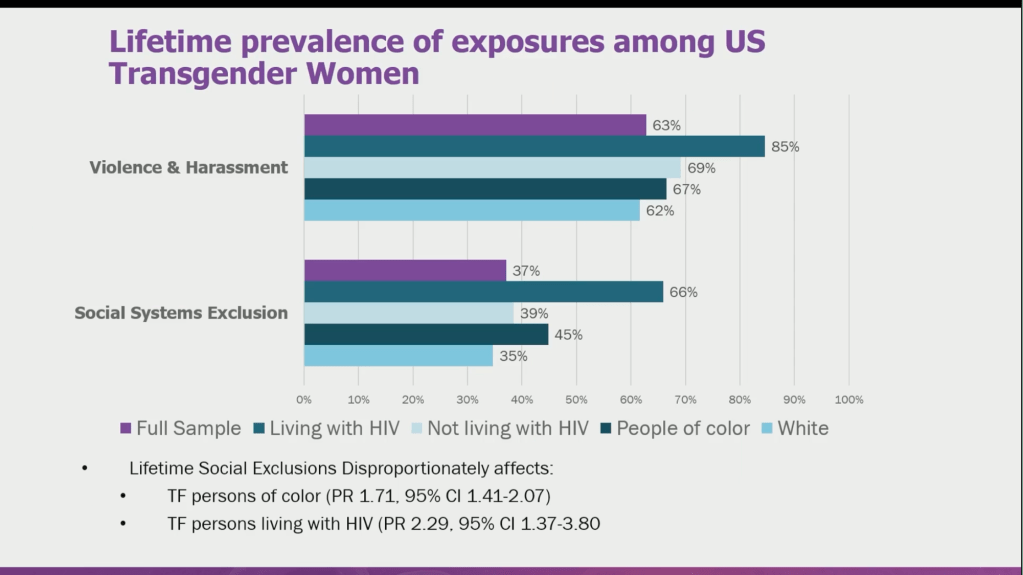
The trans content at CROI this year was somewhat underwhelming, no doubt in part due to the DEI executive orders in place. There was however an entire symposium named “Counting and Caring for Transgender and Gender Diverse Individuals.” It was sobering to see the extent of exposure to violence and social systems exclusion experienced by trans women in the US .
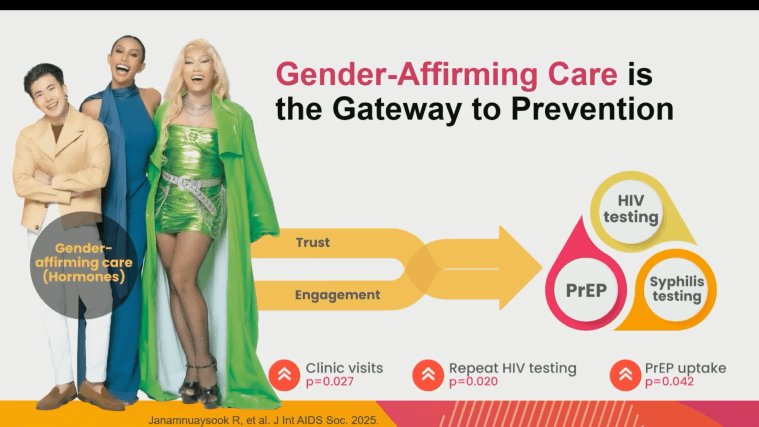
Rena Janamnuaysook from the wonderful Tangerine Clinic in Thailand reminded us of how great trans healthcare can be with a well-funded system that bundles HIV management and PrEP with gender affirming care. But the funding needs to be on a national level and not based on smaller projects with fragile funding arrangements.
This was probably for me the most disappointing study to be presented. For some time we had thought that the Meningococcal B vaccine may confer some protection against gonorrhoea, given that the organsims (Neisseria meningitidis and Neisseria gonorrhoeae) are so similar in structure. The “GoGo Vax” study was presented by Prof Kate Seib from Brisbane, where they found that 2 doses of 4CMenB vaccine 3 months apart led to no appreciable drop in cases of gonorrhoea. This may not be the end of the story, as there are other studies looking at slightly different vaccines, but for now the evidence is lacking.
It was exciting to see so many new long-acting drugs being investigated for their potential to protect HIV. Several companies have drugs under development for HIV prevention:
Cabotegravir (CAB) is the 8 weekly intramuscular injection approved by the TGA and already available in the US. Ongoing studies continue to support it as an excellent method of HIV prevention. Although not listed by our PBS at this stage, negotiations regarding pricing are occurring and I remain hopeful we may see this option in Australia one day.
Lenacapavir (LEN) as a 6 monthly subcutaneous injection has been shown to be extremely effective in 2 big trials (PURPOSE 1 and 2) for men who have sex with men, and trans and cis women. The latest updates confirm high protection after 1 year of use, with infection rates of 0.07-0.11 per 100 person years, which is far superior to oral PrEP failure rates. It also has TGA approval here, however is very expensive and unlikely to be considered for PBS listing any time soon.
A new even longer acting version of LEN which can be given as a 12 monthly intramuscular injection is now being investigated for PrEP in a new study called PURPOSE 365. Imagine that – a whole year of HIV protection from a single jab!
MK-8527 is a monthly oral PrEP pill now going through to phase 3 trials. This pill gives 1 month protection within 1 hour of the first dose (amazing), and it also has a dosing window of +/- one week. This may be a great future option for people who prefer to avoid injections and struggle with remembering pills, or are just looking for short term protection, eg “holiday PrEP”. It is also safe for use in pregnancy.
One thing to note about all the above PrEP options – none of them provide protection against Hepatitis B, unlike our current oral PrEP tablet (Tenofovir/emtricitabine or Descovy). So people going on to these options in the future will definitely need to be vaccinated if not already.
It’s clear there is a bright future for long acting HIV prevention. The challenge will be for companies to convince our pharmaceutical regulatory body that it is worth the extra cost to fund them.
Doxycycline, an antibiotic taken after sex, can decrease the risk of Chlamydia and syphilis by 80-90%. We call this Doxy-PEP (post exposure prophylaxis). San Francisco was an early adopter back in 2023, where they have seen very significant declines in these infections. There was a really interesting poster at the conference on cases of syphilis in Doxy-PEP users. The numbers were very small, as expected, but people who used Doxy-PEP and still got syphilis tended to have fewer symptoms (if any) and have much lower antibody levels (RPR titres as low as 1/2). All cases were still able to be successfully treated with a single dose of injected benzathine penicillin. This shot is a real pain in the butt, but at least we know it will still work in this scenario. If you’re on HIV PrEP you should talk with your provider about Doxy-PEP, but remember to keep having regular STI tests in case of asymptomatic infection.
The capsid inhibitor class with its show pony lenacapavir (LEN) is showing great promise for future treatments. LEN has great longevity and binds very strongly. Wes Sundquist’s plenary discussed how great a drug target the capsid really is, and I was once again entranced by the animation genius of Prof Janet Iwasa from the University of Utah. Every time I see one of her videos I just want to put a dance track to it! Watch from 6:17 for capsid action!
The 48 week results of the ARTISTRY-1 study were revealed, where people with HIV who were on complex treatment regimens were switched to a single tablet of bictegravir/lenacapavir (BIC/LEN), with reassuring non-inferiority of the new regimen, and no emergent resistance. Participants tended to be older (average age 60), with lots of comorbidities and polypharmacy, and 81% had a history of prior HIV resistance, necessitating their complex regimens. Many (70%) were on protease inhibitors at the start of the study, and had distinct improvements in their lipids after the switch. The importance of this work cannot be overstated, as there are many older people with long-term HIV who are on these sorts of complex treatments, and as their risk of cardiovascular disease increases we are constantly looking to improve and simplify their treatment without causing virological failure. Treatment resistance is always in our minds when we tamper with long-standing treatments that may be just holding things together, so a study like this showing that a switch to new drug classes maintains viral suppression is very exciting.
The combination of daily oral doravirine/islatravir (DOR/ISL) has been shown to be non-inferior to Biktarvy in a phase 3 head to head trial of people starting HIV treatment for the first time. Other studies have shown similar results for people switching off other regimens onto DOR/ISL. This adds yet another daily oral treatment option for HIV.
In an inspiring plenary, Todd Brown from Johns Hopkins University outlined what we know about this extraordinary class of drugs, the incretins, how they benefit people with HIV, and how new studies are shedding light on other unexpected health benefits.
Everyone has heard of Ozempic, the most popular injectable incretin to hit the market for diabetes management and obesity, and there are now several different incretins available, with a new oral option in the pipeline. They work by inhibiting glucagon and increasing insulin release, dropping blood sugar without causing hypoglycaemia, and at the same time causing weight loss. There is also a marked anti-inflammatory effect, which may be especially relevant to people with HIV, a virus which we know causes inflammation.
What we are now finding is that people on GLP-1s also have a huge reduction in major adverse cardiovascular events (heart attacks and strokes), a reduction in alcohol intake and smoking, and a wapping 45% drop in new diagnosis of dementia. The possibility of incretins to be used in the prevention space is obvious here.
However we need to be aware of some limitations – a possible drop in bone density in older people, and a drop in lean muscle mass. There are also common side effects, with nausea and constipation being the most troublesome, and there are some cautions regarding their use around sedation – the slowing of gastric emptying can increase the risk of gastric contents being aspirated when under anaesthetic, leading to pneumonia – so anaesthetists recommend they be stopped at least a week prior to any procedure needing sedation.
It’s worth noting that the weight loss effect with this class is subject to the rebound phenomenon, where weight piles back on if you stop the drug. Prof Brown suggested that they could be used in an induction/maintenance fashion, ie. after achieving target weight the drug is not stopped but dropped to a lower dose for maintenance of weight loss. In practice this is already how a lot of people are choosing to use GLP-1s for weight maintenance. So, TLDR version – we can’t say they are a “cure for everything” just yet, but I’m looking forward to more data, especially regarding effects on inflammation in people with HIV.
There was so much more content but I will finish here. Well done if you’ve made it to the end of this one! Stay tuned for the next update on all things HIV, sexual health and trans-related!

